
An in-depth conversation about 7-OH, high-potency kratom extracts, opioid dependence, buprenorphine, outpatient care, and the work of helping people move from daily survival toward a life they can rebuild.
For many people, the problem is no longer a search for a high. It is a life narrowed around stopping the shaking, quieting the panic, getting through work, sleeping, or feeling normal long enough to reach tomorrow.
In this conversation, Dr. Starr separates marketing language from clinical reality and brings the first question back to where it belongs: what would help this person become safe, stable, and able to begin rebuilding?
Not a perfect plan. A real next step—honest enough, medically appropriate enough, and workable enough to create a little more room for choice.

Transparency Note
I have known Dr. Ken Starr since 2015, when he was one of the first people to purchase the original version of my course, then called Ultimate Opiate Detox.
Over the years, we became colleagues and friends. I interviewed Dr. Starr twice on my former Elevation Recovery podcast and have referred certain clients to his practice when I believed their needs and circumstances appeared to fit a physician-led outpatient model of care.
I was not paid, given services, or offered any other compensation in exchange for writing or publishing this article.
The people I have referred have consistently shared that they felt respected, listened to, and well cared for. That reflects my personal referral experience, not a guarantee of outcome or a claim that this clinic—or outpatient treatment—is right for every person.
Dr. Starr reviewed direct quotations and clinic-specific clinical descriptions for factual accuracy. He did not control this article’s editorial framing, safety language, or conclusions.
This article is educational. It is not individualized medical advice, a treatment recommendation, or a detox protocol.

The One-Minute Map
If you only read one section…
take these five ideas with you:
Take These Five Ideas With You
They provide the clearest lens for understanding the rest of this article.
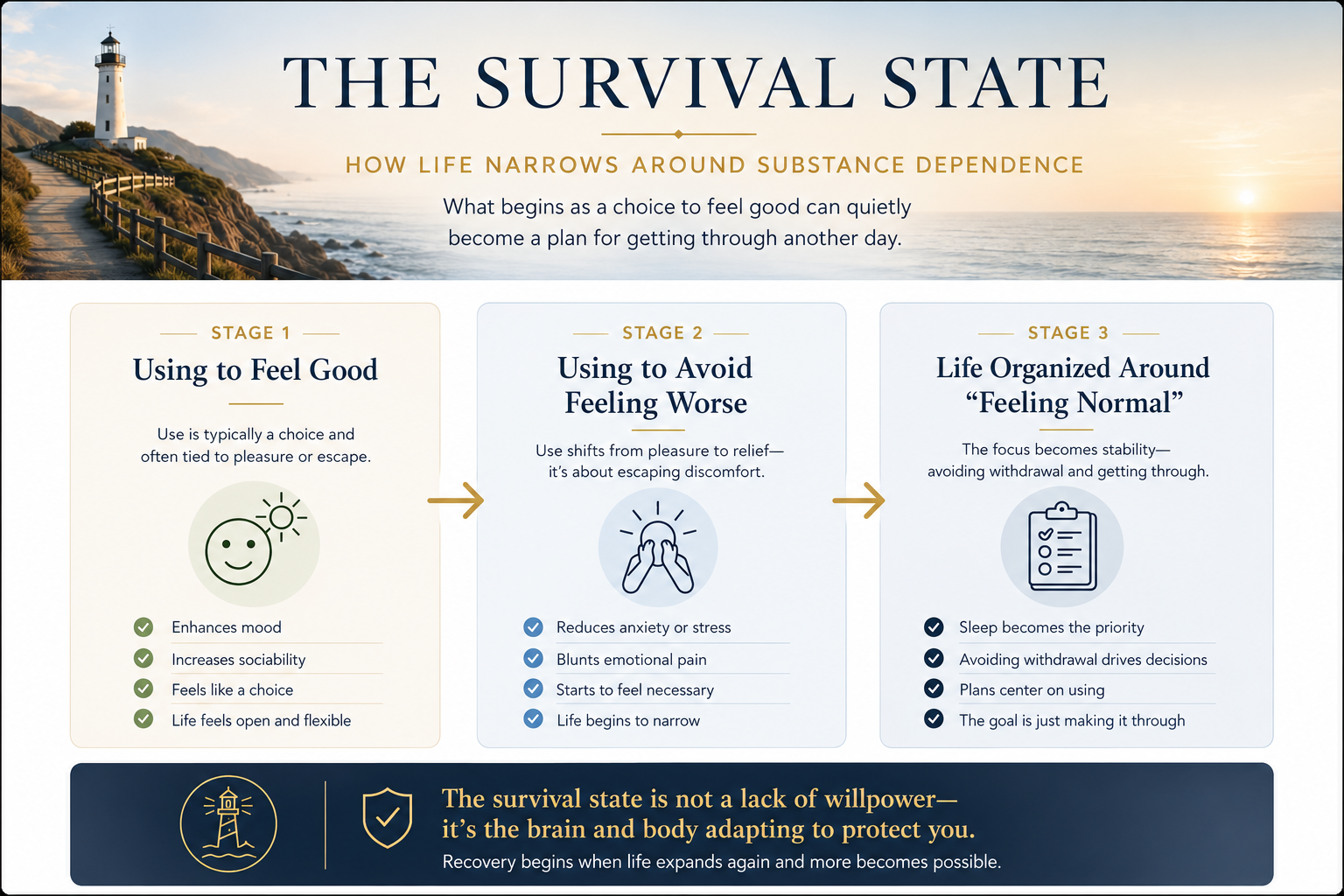
To understand why these distinctions matter, begin with the moment relief quietly becomes requirement.
What may look from the outside like a simple choice can gradually become a life organized around avoiding pain, withdrawal, and the fear of not making it through the day.
When “Feeling Normal” Becomes the Whole Goal
At first, a substance often enters someone’s life because it appears to solve a problem.
It helps them sleep.
It takes the edge off anxiety.
It makes social situations easier.
It numbs grief.
It quiets panic.
It creates energy where there was depletion.
It gives relief to a nervous system that has run out of better options.
Then, gradually, the job changes.
The person is no longer using to feel good.
They are using to avoid feeling worse.
They Are Using to Avoid Feeling Worse.
At this stage, the substance may no longer be about getting high. It may be about getting through.
For someone caught in alcohol dependence, opioid dependence, concentrated kratom extracts, 7-OH, stimulants, or another compulsive substance pattern, life can slowly narrow around one daily objective:
Get through tonight.
That is why “just stop” is such an inadequate answer.
Stopping may look simple from the outside. But when the body, nervous system, schedule, money, relationships, confidence, and sense of safety have all become organized around a substance, stopping is not merely a decision.
It is a destabilization event.
Dr. Ken Starr has spent years working in the space between two realities:
The moment when a person knows something needs to change—
and the moment when they still have no clear idea how to get safely from where they are to where they need to be.
His language for that transition is straightforward:
That is survival.
Thriving begins when life no longer has to revolve around that calculation.
Not perfection.
Not instant transformation.
But the return of time, energy, sleep, health, money, trust, dignity, and choice.
The Doctor Who Built the Care He Could Not Find
Most treatment-center stories begin with a list of services.
This one begins with a loss.
Before founding Ken Starr MD Wellness Group, Dr. Starr spent more than a decade in emergency medicine. He saw the consequences of addiction up close: overdoses, withdrawal, repeat crises, exhausted families, and people cycling through systems designed to stabilize emergencies without always creating a workable path forward.
At the same time, he watched his brother struggle with opioid addiction.
His brother later died from an overdose.
That loss is not a marketing story. It is not a credential. It is part of the reason this work became personal enough that indifference was no longer an option.
Dr. Starr also had a close friend who was among the early physicians prescribing Suboxone. He could see that medication-based treatment could create real stability. He could see people begin to function again.
But he was not seeing enough access to that kind of care in his own community.
At the time, the choices often seemed divided between two extremes:
County Services
For people with very limited resources.
Residential Programs
Expensive programs for people who could afford to step away from life for weeks at a time.
The people in the middle often had nowhere obvious to go.
Working people.
Parents.
Professionals.
People who needed privacy.
People who could not abandon their family, job, phone, or responsibilities.
People who were frightened, ashamed, outwardly functioning, and quietly running out of road.
“The middle class, the working people—they didn’t really have a place to go.”
Thus, he went to work…
So Dr. Starr rented a small office and began building what he believed should exist.
A confidential, physician-led outpatient practice where addiction could be treated as a medical, psychological, and human problem—not a moral failure.
There was no grand expansion plan.
No borrowed money.
No attempt to build the biggest facility.
He built what he believed his community needed.
And grew it organically, one patient, one family, and one hard clinical decision at a time.

The Product Changed. The Risk Changed.
The modern addiction landscape is not standing still.
Fentanyl changed it.
Designer opioids changed it.
Xylazine changed it.
And increasingly, concentrated kratom extracts and 7-hydroxymitragynine—commonly called 7-OH—are changing it too.
Packaging Is Not the Whole Story.
Part of the challenge is that the word kratom can conceal more than it clarifies.

Dr. Starr has watched this firsthand.
He has seen people arrive believing they are dealing with a relatively low-risk product because it was bought openly, marketed casually, or framed as a safer alternative.
Then the actual pattern of use comes into view:
Tolerance.
Withdrawal.
Escalating cost.
Hidden use.
Fear of running out.
A life that begins to revolve around avoiding sickness.
“Honestly, I’ve learned more from patients than from textbooks.”
That is not an argument against science.
It is a reminder that addiction medicine must remain awake.
A textbook can tell you what a molecule is.
A patient can tell you what it is doing in real life.
They can tell you when the product they are buying has changed.
They can tell you when the old amount no longer touches withdrawal.
They can tell you when they are waking up sick.
They can tell you when they are hiding use from a partner, draining savings, missing work, or using simply to feel normal enough to participate in their own life.
Those experiences are not noise around the data.
They are often the earliest signal that the clinical reality is shifting faster than public understanding.
The Better Questions
The question is not simply:
“Is kratom good or bad?”
The better questions are:
The Better Questions
Before deciding what kind of help may be needed, start by getting clear on the pattern itself.
Those questions move the conversation away from ideology and toward reality.
And reality is where responsible treatment begins.
The First Question Is Safety, Not Sales
A responsible first call should not feel like a sales conversation.
It should feel like a safety conversation.
The first question is not:
“Which treatment package should this person choose?”
It is:
“What level of care gives this person the best chance of getting safe?”
That distinction matters.
When someone reaches out to Dr. Starr’s practice, the goal is to understand the full situation before deciding whether outpatient care is an appropriate fit.
That means looking beyond the substance.
It means considering:
Current pattern of use
Withdrawal history
Other medications or substances involved
Medical conditions
Psychiatric complexity
Prior treatment attempts
Stability at home
Available support
Ability to attend appointments and follow through
Whether the person can remain safe outside a hospital or residential setting
What they can realistically afford and sustain

This is where clinical honesty matters.
Outpatient care can be deeply meaningful for the right person. It can preserve privacy, work, family connection, daily structure, and autonomy while still offering medical oversight and accountability.
But outpatient care is not appropriate for everyone.
Dr. Starr described a patient who needed to return for alcohol detox but could not get to the clinic sober.
That is not a failure of character.
It is clinical information.
It may mean that residential, hospital-based, or more medically supervised care is the safer next step.
“A higher level of care isn’t a failure—it’s the appropriate clinical decision.”
Too many people treat level of care as a referendum on strength.
It is not.
It is a question of risk, support, medical need, and what the person can safely manage right now.
Stability Before Skills
One of the most persistent misunderstandings in opioid treatment is the idea that buprenorphine is simply “trading one drug for another.”
That phrase turns a clinical question into a moral argument.
It also misses what medical stabilization can make possible.
Dr. Starr does not describe buprenorphine as the end of recovery.
He describes it as a potential foundation for recovery. [2]
“It creates medical stability that allows people to develop the recovery skills they’ll carry forward.”
That distinction is everything.
When someone is cycling through withdrawal, cravings, panic, pain, insomnia, secrecy, financial pressure, and the relentless logistics of finding and using a substance, they may have very little capacity left for deeper work.
It is hard to repair a relationship when you are trying not to get sick.
It is hard to build routines when your nervous system is in emergency mode.
It is hard to think long-term when every few hours feel urgent.
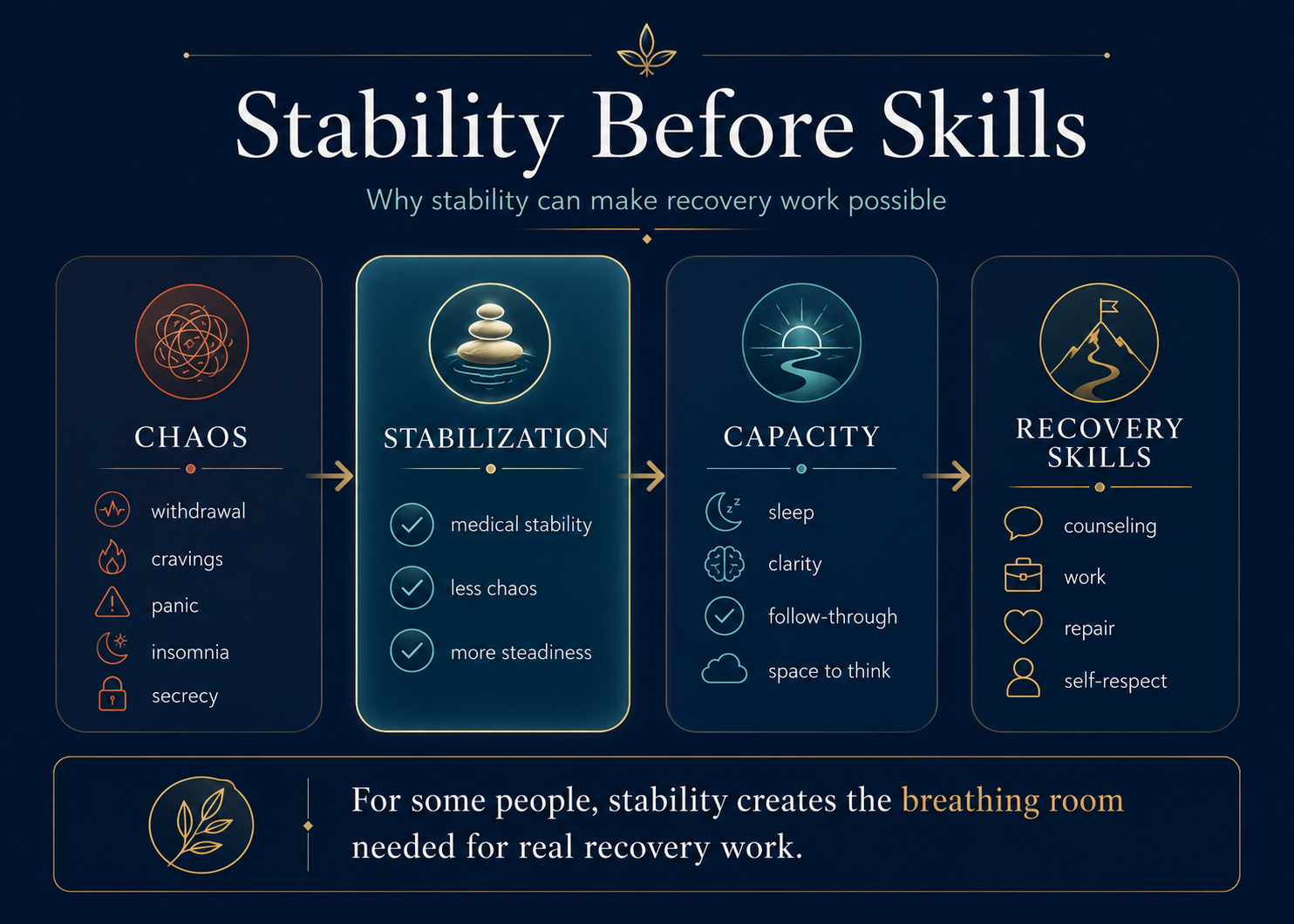
For some people, clinician-guided buprenorphine treatment can create a decision window.
A little more time between panic and action.
A little more sleep.
A little more steadiness.
A little more capacity to attend counseling, return calls, eat, work, repair trust, move their body, and begin rebuilding self-respect.
That does not make medication a cure.
It does not mean every person should use medication.
It does not mean every person should stay on it for the same length of time.
It means that for some people, medication can reduce chaos enough for recovery to become possible.
The Goal Is Not a Medication Ideology
Dr. Starr’s work is not built around a rigid medication philosophy.
It is built around asking:
What has worked before?
What has not?
What is the person’s actual risk?
What can they sustain?
What will give them the greatest chance of building a life beyond daily survival?
Long-acting injectable forms of buprenorphine, including Sublocade and Brixadi, can be useful clinician-guided tools for some patients. For others, they may not be the right fit.
The point is not to make one medication sacred.
The point is to create enough stability for a person to begin becoming free.
Boulder QuickStart: A Launchpad, Not a DIY Shortcut
Dr. Starr also uses what he calls the Boulder QuickStart — a clinician-managed strategy intended to help certain patients move from active opioid use into buprenorphine treatment in a compressed timeframe.
For the right person, that can lower a major barrier to getting started.
Instead of spending days trapped between continued use and a difficult transition, a patient may be able to enter stabilization more quickly under medical supervision.
But this needs to be said without ambiguity:
A faster transition is not a home protocol.
It is not a social-media hack.
It is not a set of instructions to copy from a blog post.
It is not a reason to self-manage a complex opioid transition without medical assessment and oversight.

A method can sound simple in one sentence while still requiring substantial clinical judgment, symptom management, monitoring, and individualized decision-making.
The point is not speed for its own sake.
The point is making a safer beginning more accessible for the right patient.
Build the Plan Around a Real Life, Not an Ideal One
One of Dr. Starr’s strongest themes is that treatment has to be realistic.
Not idealized.
Not designed for a hypothetical person with:
- Unlimited money
- Unlimited time
- Perfect support
- No responsibilities
- No fear
Real people have jobs.
They have children.
They have debt.
They have transportation limitations.
They have strained relationships.
They have medical conditions.
They have shame.
They have lives that may already feel one mistake away from collapse.
A recovery plan that cannot survive a person’s real life is not a recovery plan.
It is a wish list.
That is why Dr. Starr begins with a conversation rather than a prepackaged answer.
What has worked before?
What has failed?
What can the person afford?
What can they realistically commit to?
What support exists outside the clinic?
What symptoms can be managed safely?
What additional resources would genuinely help?

A treatment plan may include one or more of the following:
Medication management
Counseling
Education
Wellness care
Neuromodulation
NAD+ therapy
Supportive infusions
Outside referrals
But the value is not in how many services can be listed.
The value is in whether the pieces fit together.
Whether they are safe.
Whether they are proportionate.
Whether they respect the person’s budget.
Whether they help the person build a life instead of merely endure another week.
The best plan is not the most impressive plan on paper. It is the safest plan a person can actually live.
That is individualized care.
Small on Purpose
Dr. Starr’s practice is small by design.
When someone comes to the clinic, they are not entering a large anonymous system where every appointment begins with another introduction and every decision passes through layers of distance.
Dr. Starr is the owner.
He is present.
He is accountable.
“When patients come here, they see me. I’m the owner, I’m present, and I’m accountable.”
That matters.
Not because every large program lacks humanity.
Not because every small practice is automatically better.
But because addiction treatment is deeply personal.
People often arrive ashamed.
They may not trust doctors.
They may have been dismissed.
They may have been lectured.
They may have been told to “just stop.”
They may have been treated as a liability, a diagnosis, a relapse risk, or a problem to manage.
Being known can matter.
Being able to ask a question without feeling like a burden can matter.
Being told honestly, “We can help with this,” or, “This is beyond what can be safely managed here,” can matter.
In addiction care, dignity is not a soft extra.
It is part of the infrastructure.

Dignity Is Not a Tagline
Dr. Starr’s brother’s overdose death is not presented here as a branding story.
It is the personal loss that shaped the standard of care he wanted to create.
His mission is plain:
That principle shows up in practical ways.
It shows up in whether a person is treated with respect after a return to use.
It shows up in whether a family receives honest guidance rather than vague reassurance.
It shows up in whether a clinician can hold a firm line when a higher level of care is needed.
It shows up in whether treatment is built around the person rather than around a generic protocol.
It shows up in whether someone is allowed to be complicated.
Because people are complicated.
Dependence is complicated.
Recovery is complicated.
And shame does not make anyone easier to reach.
Questions to Ask Any Addiction Treatment Provider
Whether someone is considering Dr. Starr’s practice or another program, these 10 questions are worth asking:
Ten Questions Worth Asking
A strong provider should welcome these questions and answer them plainly.
What level of care do you believe I need, and why?
What medical or withdrawal risks concern you most in my situation?
What would make you recommend inpatient, residential, or hospital-based care instead?
How do you individualize medication decisions?
What happens after detox or initial stabilization?
What is the plan if symptoms worsen or the original plan is not enough?
What is the realistic cost, timeline, and follow-up plan?
How will you coordinate with my other clinicians, therapist, family, or support system when appropriate?
What does success realistically look like in the first week, first month, and first six months?
What happens if I am not a fit for this level of care?
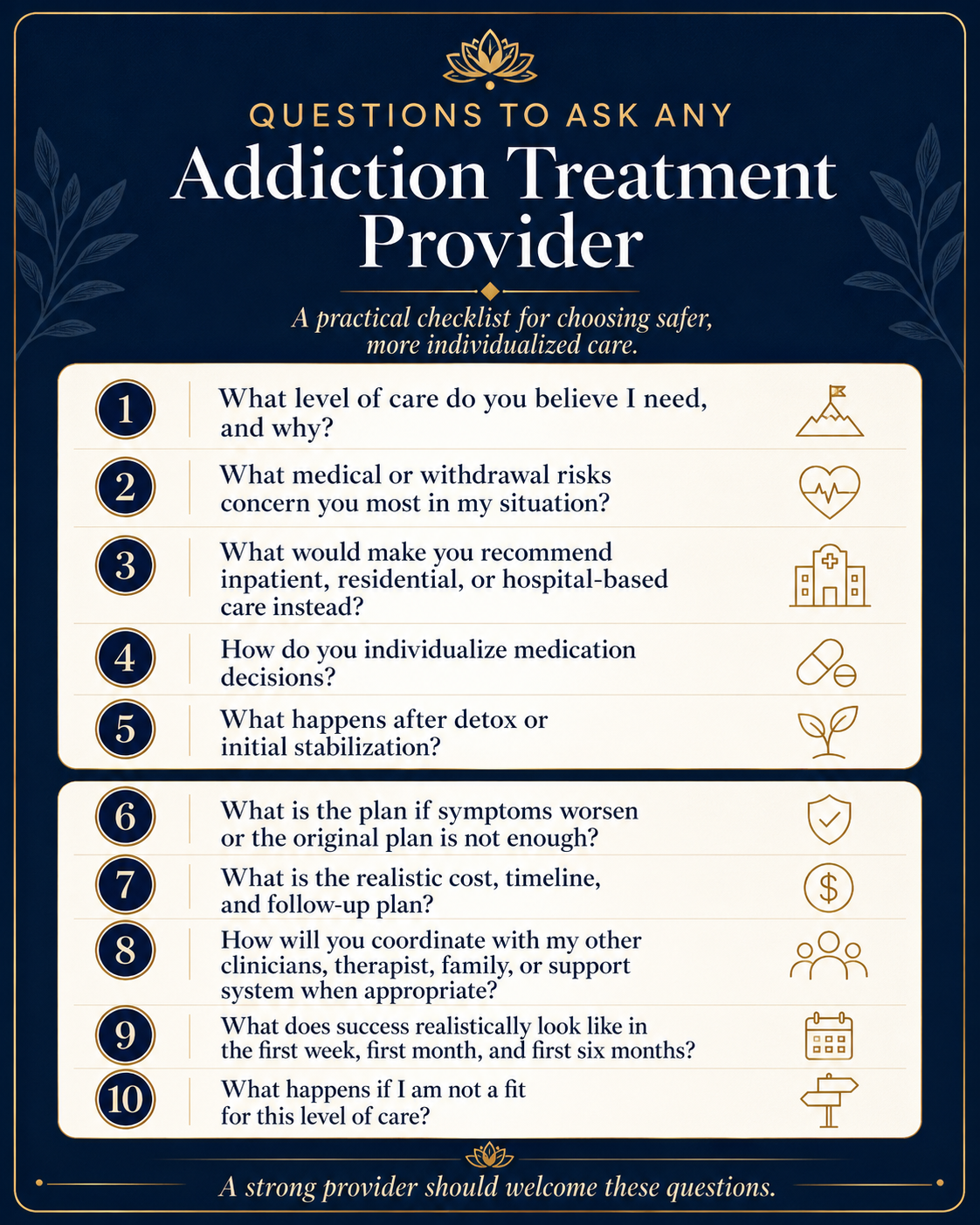
A strong provider should welcome these questions.
Frequently Asked Questions
Grounded answers for people trying to understand 7-OH, kratom extracts, withdrawal risk, medication support, and what a safer first step can look like.
“`01 Is 7-OH the same thing as traditional kratom leaf?
No. The broad word “kratom” can conceal meaningful differences. The FDA notes that 7-OH occurs naturally in trace amounts in the kratom plant, while its warning focuses on products containing 7-OH as an added ingredient or at enhanced levels.
SOURCE NOTE [1] ↗02 Are all products sold as “kratom” interchangeable?
No. A casual retail setting, bright package, or botanical-looking label cannot tell you the whole clinical story. Start with better questions: What is in the product? What does the label say? How often is it used? And what happens when the person tries to stop?
SOURCE NOTE [1] ↗03 Does medication support mean someone has failed at recovery?
No. For some people, medication support creates enough stability to sleep, think, work, repair relationships, and participate in the rest of recovery. SAMHSA describes buprenorphine as a medication for opioid use disorder that should be prescribed as part of a comprehensive plan that includes counseling and other services.
SOURCE NOTE [2] ↗04 Can this article be used as a self-detox plan?
No. This resource is designed to help a person recognize the pattern, ask better questions, and identify safer next steps. It does not replace an individualized medical assessment—especially where alcohol, benzodiazepines, opioids, significant medical conditions, or multiple substances are involved.
05 When should someone seek urgent or higher-level care?
Seek urgent medical help for severe confusion, hallucinations, seizures, loss of consciousness, difficulty breathing, chest pain, extreme agitation, or immediate danger to self or others. Alcohol withdrawal can be medically dangerous and should be assessed by a qualified clinician.
SOURCE NOTE [3] ↗06 What should I ask a treatment provider before committing?
Ask how they assess safety, what level of care they recommend and why, how they handle withdrawal risk, whether medication support is available when clinically appropriate, what the schedule and total cost are, and what happens after the first phase of care. See the full provider-question checklist.
07 What is a realistic first step today?
Start smaller than the whole future: one honest conversation, one call, one appointment request, one medical assessment, or one person who finally knows what is happening. The goal is not perfection. It is enough safety and choice to take the next right step.
Beyond Getting Through Tonight
For someone caught in dependence, the word thriving can sound almost insulting at first.
Too far away.
Too polished.
Too unrealistic.
When a person is trying not to get sick, survive a night of cravings, manage panic, hide use, repair a relationship, or simply get through work, thriving may not feel like the next step.
And maybe it is not.
Maybe the next step is one safe night.
One honest conversation.
One medical assessment.
One person finally telling the truth.
One plan realistic enough to follow.
One week of stability.
One morning where the entire day is not organized around a substance.
Recovery does not have to begin with a grand declaration.
Sometimes it begins with the return of a little room.
Room to sleep.
Room to eat.
Room to think.
Room to return a call.
Room to work.
Room to tell the truth.
Room to discover that the substance is no longer the only thing holding life together.
The opposite of survival is not perfection.
It is the return of choice.
And that is where rebuilding begins.

Ken Starr MD Wellness Group at a Glance
Explore the clinic’s current information, learn more about its story, or contact the practice directly.
107 Nelson St, Arroyo Grande, California 93420
Visit the Website
Review current practice information, services, and contact details.
Read Our Story
Learn more about the values and philosophy behind the practice.
Call the Office
Reach Ken Starr MD Wellness Group directly by phone.
Email the Practice
Use email for general inquiries and direct communication.
The clinic’s website currently lists outpatient medical detox and stabilization, intensive outpatient detox, intensive outpatient recovery, outpatient recovery, counseling-related support, and wellness services.
Important Safety Note
This article is not a self-detox guide.
Do not use it as a substitute for medical assessment, especially for alcohol dependence, benzodiazepine dependence, opioid dependence, or polysubstance use.
Alcohol withdrawal can be medically dangerous. [3] Benzodiazepine withdrawal can also be medically dangerous and warrants medical assessment. Severe confusion, hallucinations, seizures, loss of consciousness, difficulty breathing, chest pain, extreme agitation, or immediate danger to self or others require urgent medical attention.
Call emergency services or go to the nearest emergency department if someone may be in immediate danger. If a person is unresponsive after using a substance, call 911 immediately.
Source Notes
[1] U.S. Food and Drug Administration. Products Containing 7-OH Can Cause Serious Harm.
[2] Substance Abuse and Mental Health Services Administration. What Is Buprenorphine?
[4] Ken Starr MD Wellness Group. Current published program, contact, and location information.
[5] Written interview responses from Dr. Ken Starr, reviewed for quote and clinic-specific factual accuracy; edited only for length and clarity.
Leave a Reply